He Said
The concept of National Childhood Obesity Awareness Month is flawed in several ways, many of which Joanne covers in her She Said passage. The most glaring issue, in my opinion, is that by promoting the use of weight as a proxy for health, the government is paradoxically distracting from matters of actual health.
Human beings can be healthy at a variety of weights, which is why we cannot draw accurate conclusions about someone’s health or behaviors based solely on their size. Thin folks can have plenty of medical woes. A couple of years ago, I wrote about a slender friend of mine who was diabetic, suffered a heart attack, and ultimately died of cancer. Someone might be thin due to food insecurity, a medical condition, psychological disturbances, eating disorders or disordered eating, or overexercise, just to name a few of the health-threatening issues that might lead to lowered body weight.
With a focus on obesity, not only do we miss an opportunity to identify and assist people at risk for or suffering from these problems, but we actually push them in the direction of trouble. For example, I have recently seen an increase in pediatric patients, including males, with eating disorders or disordered eating that reportedly stemmed from a fear of getting fat brought on by discussions at school or the doctor’s office.
One of my teenage patients recently told me how his pediatrician praised him for having lost weight from one annual checkup to the next after having chastised him the year before, but what his doctor did not know was that my patient had overexercised and restricted his food intake leading up to the appointment for fear that his doctor would again be mad at him if he had not lost weight. My patient’s behaviors brought him further away from health, not towards it, and the poor communication between him and his doctor puts him at risk for improper care in the future. Furthermore, food restriction elevates his risk for binge eating disorder and, ironically, ultimate weight gain.
Trust me, children who are obese already know it. They hear about it on the playground, in gym class, on television, online, maybe in the pediatrician’s office, and from other sources that tell them something is wrong with their bodies and it is their fault. National Childhood Obesity Awareness Month calls even more attention to them and their bodies, thereby exacerbating stigmatization and bullying.
The concept of National Childhood Obesity Awareness Month may be well intentioned, but its fallout is the exact opposite of the desired effect. If we want to improve the actual health of our children, better to promote size diversity and the importance of healthy behaviors, such as fun and appropriate physical activity, for everybody.
She Said
According to the U.S. Department of Health and Human Services (HHS), September is National Childhood Obesity Awareness Month. Per the HHS website, “one in 3 children in the United States are overweight and obese,” putting kids at risk for developing health problems such as type 2 diabetes, hypertension, and heart disease. The website goes on to say that childhood obesity is preventable, as “communities, health professionals, and families can work together to create opportunities for kids to eat healthier and get more active.” Some of the strategies that the HHS recommends are nutrition based, such as “keeping fresh fruit within reach” and providing healthier food options at school, and other strategies are focused on activity levels, such as encouraging families to go on an after-dinner walk and incorporating daily physical activity at school.
While I actually applaud the strategies put forth by the HHS to improve kids’ health, I am saddened to see the focus be on body size. Thanks to Michelle Obama, childhood obesity is at the forefront of the American consciousness. Kids are being weighed and measured at school and then later sent home with a health report card telling them whether they are at a “healthy” body mass index (BMI) or are in the “overweight” or “obese” categories. Even though the medical community as a whole willingly acknowledges that the BMI is woefully flawed as an indicator of health status, it still condones its use in determining the health of our kids. Time and time again, studies have shown that behaviors rather than weight are a better determinant of health, but unfortunately, this is not being reflected in current policy.
My greatest concern is the effect that focusing on childhood obesity could be setting up kids to develop eating disorders (EDs). I cannot tell you how many preteens who have stepped into my office had been sent home with their BMI report card and then developed either extremely disordered eating or an actual diagnosable ED. What often happens is that the parents become alarmed at their child’s negative BMI report and will start to impose harsh diet restrictions and exercise ultimatums. I had one patient whose father promised her and her sister iPads if they both lost weight. Not only would he limit their access to “junk” food, he would make them run laps around their neighborhood after dinner every night. As a result of this, the patient developed a very disordered relationship with food and her body. This story is not unique, unfortunately. I have heard it too many times to count.
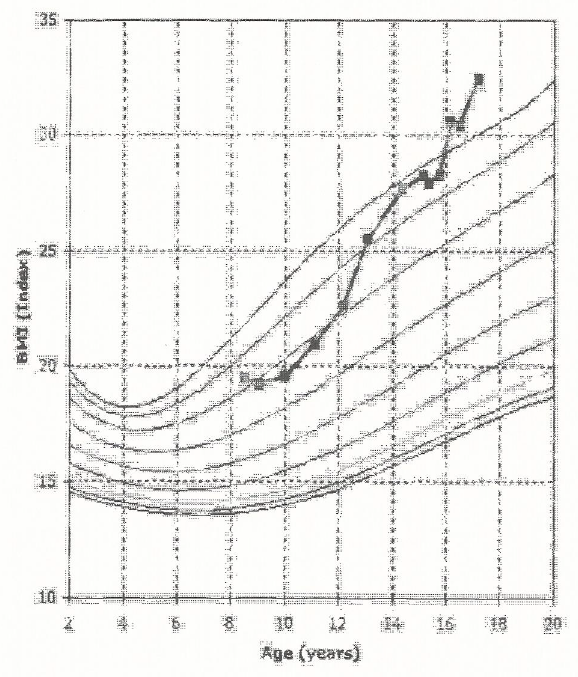
So, I have a few issues with the HHS’s focus on obesity. First of all, I don’t believe that we should have schools be weighing and measuring kids and sending them home with a BMI report card. Instead, the child’s pediatrician and parents should be the gatekeepers of the child’s health. Every child has their own unique growth charts – some trend on the higher end of weight for height, while others trend on the lower end of the chart. In other words, some kids are just meant to be in bigger bodies, while others are meant to be in smaller bodies. These body sizes do not tell us anything about the child’s health unless there are major changes in either direction. For instance, one would expect a child trending on the 85th percentile to stay at that percentile. If there was a sharp drop to the 50th percentile, that would be cause for concern. Similarly, if a child was trending on the 50th percentile and then jumped up to the 90th percentile, that should also be looked at. One body type is not inherently healthier than the other – every body is unique.
In addition, I think it is so important to not speak negatively about a child’s weight. Kids are like sponges, and they pick up on everything. Talking with one’s child about how their body works and teaching them how to take care of it is one thing, but telling a child that they are too big and need to lose weight is extremely damaging and can set the child up for years of negative body image and a life of disordered eating. Many EDs start when a well-meaning parent tries to teach their child to diet and use exercise to burn calories. In fact, there are a number of studies that show that when children are put on restricted diets, they will often end up being heavier adults.
Also, I think that if a parent has concerns about his or her child’s weight, they should talk with their child’s pediatrician separately (i.e., not with the child in the room). Instead of telling the parent that their child simply needs to lose weight, it would be wonderful if pediatricians did not just make an assumption based solely on the child’s weight that the child is engaging in unhealthy behaviors. If it is determined that the child is in fact not practicing healthy lifestyle behaviors, it would be best if the doctor just focused on helping the child develop these healthy habits (perhaps by referring them to a registered dietitian or other health care provider) and measure the child’s progress by their weight.
Given that, I don’t think that National Childhood Obesity Awareness Month is helpful at all in helping our kids lead healthier lives. By teaching them that weight is synonymous with health, we are doing them a major disservice. Perhaps September could instead be called National Healthy Habits Awareness Month? Just a thought.