He Said
Wellness class. The other freshmen and I thought the class was such a joke that if you told then-15-year-old Jonah that in a couple of decades he would wittingly choose to incorporate the word “wellness” into his business’s name, the cognitive dissonance would have rocked his adolescent world view.
Wellness class was gym without the, well, gym. The teachers were the same, but instead of leading us through units of volleyball, basketball, and badminton, they taught us about health and nutrition. The overarching culture, however, was consistent. Gym was the informal time of day, the high school version of recess. It was a time to let loose, move our bodies to one extent or another, and measure ourselves against our peers, both figuratively and, as you will read, sometimes literally. You had better believe the spirit of competition bled into the wellness classroom, too.
Even at 15, I could tell that the school’s approach to wellness was off base. We used to undergo various exercise performance tests (pull-ups, submaximal cycle ergometer, sit-and-reach) as well as anthropometric exams (weight, height, body composition). All of these evaluations happened in front of the group, so we all knew how each of our peers had fared. Gee, sounds like a great plan; what could possibly go wrong?
After the testing was over and it came time for the teachers to gather us together and offer congratulatory certificates to those of us who had what I suppose were good results in the eyes of the teachers or whatever norms against which they measured us, I crumpled up my award in my hands on the spot. Immediately, I felt guilty as if I had disrespected the teachers who had given it to me, but as time went on, I confirmed that my intuition was right.
If the teachers gave some of us certificates based on our body measurements, what kind of message did they send to all of the other students who did not receive such certificates? As a result, how do you think those students felt about themselves and their bodies? Similarly, how do you think their certificate-holding peers viewed them? The teachers indirectly started the bullying by posting their body mass indices and body composition results, thereby publicly shaming them, and other kids were more than happy to pick up the harassment where the teachers left off.
See, here’s the thing: If a teacher is conveying oversimplified and misguided lessons about how we can manipulate our bodies and our weight based on how we eat and exercise, and then they single out the kids whose bodies happen to be larger, the message they are indirectly teaching is that something is wrong with these larger students, that they are not doing enough to take care of themselves, that they are lazy and/or eat too much. And we wonder how weight stigma forms and gets perpetuated.
I still remember two of the largest kids in my class as well as their body composition results. These data should never have been my business to know. What does it say about the culture the school created that these results have stuck with me all this time? That was not wellness.
If we are going to even consider teaching nutrition in schools, we have to scrap the status quo and reexamine fundamental questions of who will do the teaching, what expertise do they hold, what environment will they create, will they reinforce stigma or break it down, and most importantly, what lessons will students actually absorb about their relationships with food, physical activity, and their bodies. If we cannot provide answers that are worthy of their own certificates of satisfaction, then we should not be teaching nutrition in schools at all.
She Said
As the holidays have come to a close, it’s back to reality for most of us. For some of my patients, that means back to school. Lately, it seems like I have been hearing a lot about school-based nutrition programs from my patients. Some of these programs are being run in their health classes, while others are part of their biology curriculum or other classes. It got me thinking about the subject of nutrition and school. Should nutrition be taught in elementary, middle and high schools? If so, who should be teaching it to the students? What should the nutrition course cover?
Given that the vast majority of my patients are those struggling with eating disorders, I have some mixed feelings about nutrition in school. On the one hand, I think it’s important for kids to learn about how to take care of themselves and the consequences of their lifestyle choices on their health. For instance, it makes sense to me for kids to learn about different nutrients and how they can help them grow and thrive.
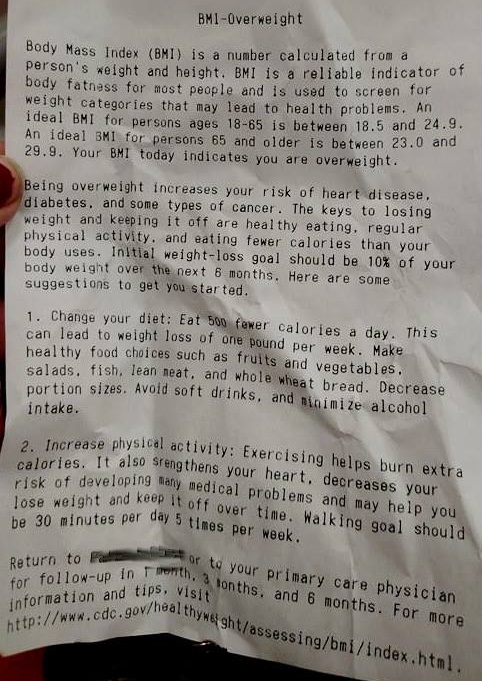
But I worry that along with this helpful information, the kids might be learning a whole different lesson. From what I’ve heard, many of these nutrition programs are focused on making sure students maintain a healthy weight and actually scare them about the potential dangers of being overweight. As Jonah and I have written about extensively, health and weight are not synonymous; lifestyle behaviors are a much better predictor of health outcomes. This means that even if someone falls into the “overweight” or “obese” categories on the BMI scale, they are not necessarily doomed to poor health. Similarly, someone who falls into the “normal” weight category might not be healthy. It’s the behaviors that make the difference, not weight.
In addition, kids (and adults) come in a wide array of sizes and body types – we are not all meant to be slender. Genetics are a huge determinant of body weight. And as we have noted many times before, diets (or any program or restrictive way of eating meant to alter one’s body size) fail 95% of the time, usually ending up in weight regain. Oftentimes, I hear that school nutrition programs propagate the false idea of “calories in, calories out” in regards to weight. It’s just not that simple.
Unfortunately, the main message that most of my patients glean from these school nutrition programs is “fat = bad” and “these are the foods to avoid in order not to be fat.” In one case, one of my patients told me her biology professor had her students calculate their resting metabolic rates and then keep a food journal to log their calories to later evaluate if they were eating too much to maintain their weight. Another one of my patients told me that she actually learned about eating disorders from an educational video shown in her health class and that’s when her bulimia started. For someone who has the genetic predisposition for developing an eating disorder, these types of messages and activities can actually trigger them to start restricting.
What’s the solution to this problem? One thought I had is that schools could hire a registered dietitian as a nutrition consultant who is well versed in eating disorders and Health at Every Size®. Perhaps that dietitian could run a nutrition program for the students or train teachers to do so. Ideally, I would think the program should be focused on being weight-neutral, helping students embrace a variety of body types and sizes, and not advocating for restricting certain foods. In addition, maybe it would be a good idea to make nutrition programming an optional part of the school curricula, as some parents might not want their child to learn about nutrition in school. Perhaps the nutrition course could be offered as a voluntary program after school hours for those who are interested in it. I’m not sure what the right answers are to these questions, but I hope that as our society becomes more educated about health and weight, things will change in our schools.